Hashimoto’s disease
Exploring new approaches to help with Hashimoto’s disease
Low-dose naltrexone (LDN) may help calm the immune system in Hashimoto’s disease.
Compounded LDN available in liquid, capsules and buccal form. Please complete the consultation to view LDN compounded solutions.
Important
Compounded treatments, eg, LDN, ED patches, Melatonin, or for hair loss, are visible after completing a consultation. If you have previously purchased, you can reorder from your account.
What you should know about Hashimoto’s disease
Hashimoto’s disease is an autoimmune condition where your immune system mistakenly attacks your thyroid gland. Over time, this can damage the gland and lead to low thyroid hormone levels (hypothyroidism).
Hashimoto’s can affect anyone, but it’s much more common in women—10 to 20 times more likely than men—and can develop at any age, even in children.
Common symptoms include tiredness, weight gain, feeling cold, constipation, dry or rough skin, thinning hair, low mood, memory problems, and sometimes swelling in the neck (goitre).
Doctors diagnose Hashimoto’s by checking your symptoms, running blood tests for thyroid hormones (TSH, free T4, free T3) and antibodies, and sometimes doing an ultrasound of your thyroid.
Yes! Early on, as the thyroid is attacked, stored hormones can leak into your blood, causing temporary high levels (hyperthyroidism). Over time, the thyroid can’t keep up, and you develop hypothyroidism.
The main treatment is a daily tablet of levothyroxine (T4), a synthetic thyroid hormone. Your doctor will adjust your dose based on regular blood tests and how you feel.
T3 is not routinely prescribed in the UK due to limited evidence of benefit, possible side effects, and higher cost. Most people do well on T4, but a small number may need combination therapy.
LDN is being explored as a complementary therapy due to its modulating effect on the immune system. Some people report feeling better, but scientific evidence from large-scale trials is lacking. It’s generally safe and may be worth considering if you’re not feeling your best on standard treatment.
Additional information
Hashimoto’s disease
Hashimoto’s disease is an example of an autoimmune condition where the body produces antibodies that attack the thyroid gland tissue, slowly destroying it, causing hypothyroidism, or low thyroid levels [1], [2].
Hashimoto’s thyroiditis is one of the most common hormone-related (endocrine) conditions around the world, affecting about 1–2% of people [3]. It can develop at any age—including in children—but it’s much more common in women than men, with women being affected 10 to 20 times more often [2].
Before we explore Hashimoto’s disease in more detail, let’s first focus on the thyroid gland itself and why it is so important.
The small but powerful thyroid gland
The thyroid gland is a small, butterfly-shaped organ located at the front of the neck. It is responsible for the production of the thyroid hormones, which are crucial for several important functions in the body, such as [4]:
- Regulating your metabolism (how your body turns food into energy)
- Controlling your body temperature
- Managing your heart rate and how strongly your heart beats
- Supporting normal growth and development in children
- Helping your brain and nervous system work properly
- Influencing your mood and mental wellbeing
- Supporting muscle strength and function
- Regulating how quickly your body uses oxygen
- Helping to maintain healthy skin, hair, and nails
- Supporting digestion and how quickly food moves through your gut
- Helping to control cholesterol levels
- Supporting menstrual cycle regularity and fertility
In fact, there is not a single cell in the body that does not rely on the thyroid hormones in some way, so you can see that when something goes wrong, it can have huge repercussions for the whole body.

Hypothyroidism
Hypothyroidism occurs when there are low levels of thyroid hormone. This produces the following symptoms [5]:
- Fatigue or feeling unusually tired
- Weight gain despite no change in diet
- Feeling cold or having cold intolerance
- Constipation
- Dry, rough skin
- Hair thinning or hair loss [6]
- Loss of the outer third of the eyebrows [6]
- Slow heart rate
- Depression or low mood
- Memory problems or difficulty concentrating (sometimes called “brain fog”)
- Hoarseness or a deepened voice
- Puffy face or swelling, especially around the eyes
- Muscle weakness or cramps
- Joint pain or stiffness
- Slow reflexes
- Menstrual irregularities or heavy periods
- Puffy or swollen thyroid gland (goitre)
- Enlarged tongue
- Puffy hands and feet
- Slow speech or thinking

Hyperthyroidism
This occurs when excessive amounts of thyroid hormones are released from the thyroid gland. This produces the following symptoms [7]:
- Unexplained weight loss despite normal or increased appetite
- Rapid or irregular heartbeat (palpitations)
- Feeling hot or heat intolerance
- Increased sweating
- Nervousness, anxiety, or irritability
- Tremors (shaking hands or fingers)
- Difficulty sleeping (insomnia)
- Muscle weakness, especially in the upper arms and thighs
- Frequent bowel movements or diarrhoea
- Thinning skin or fine, brittle hair
- Enlarged thyroid gland (goitre)
- Bulging eyes (Graves’ ophthalmopathy)
- Menstrual irregularities or lighter periods
- Fatigue or muscle weakness
- Increased sensitivity to light and eye irritation
- Rapid speech or difficulty concentrating
Autoimmune thyroiditis
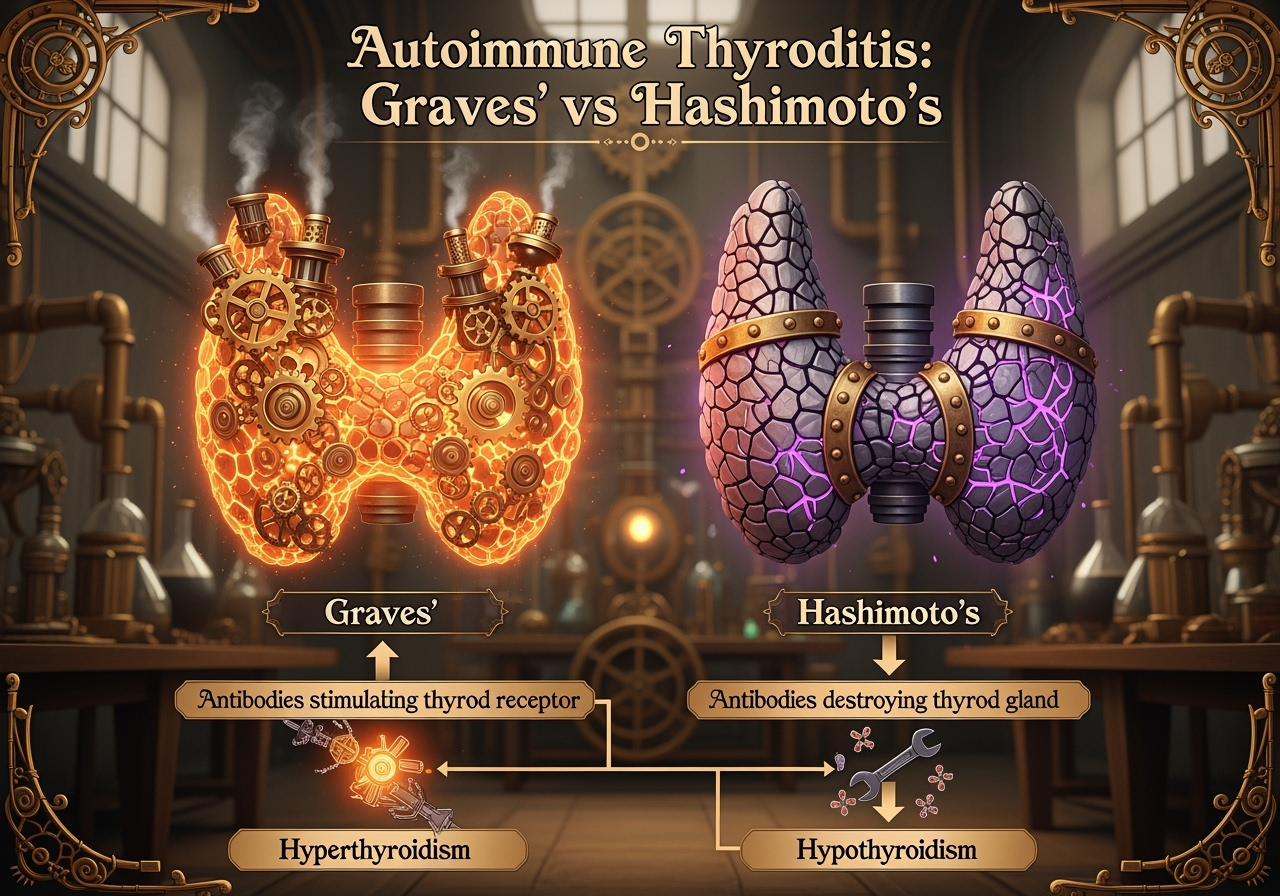
When the immune system attacks the thyroid gland, it can cause either Graves’ disease or Hashimoto’s disease.
In the case of Graves’ disease, the immune system produces antibodies that stimulate the thyroid receptor, resulting in hyperthyroidism (excessive production of thyroid hormone) [8]. In Hashimoto’s disease, the immune system makes antibodies which slowly destroy the thyroid gland, leading to hypothyroidism with low levels of thyroid hormone [2].
Hashimotos disease
In Hashimoto’s disease, the immune system gradually destroys the thyroid gland, resulting in lower levels of circulating thyroid hormones. However, many people newly diagnosed with Hashimoto’s disease will experience many symptoms of both high and low levels of thyroid hormones. What’s going on?
As the thyroid gland is attacked and damaged by the immune system, thyroid hormones that are typically stored inside the cells are released into the bloodstream, leading to elevated levels of thyroid hormones. This causes a transient hyperthyroid state and may even lead to toxic levels of these hormones, called thyrotoxicosis [9]. Eventually, the extra hormone is cleared out of the body, resulting in a hypothyroid state as the damaged thyroid gland struggles to produce enough thyroid hormone to meet the body’s demands.

Thyroid feedback system
Before examining how Hashimoto’s disease is diagnosed, it is essential to understand how the body regulates thyroid hormone levels.
Understanding the feedback system for thyroid function
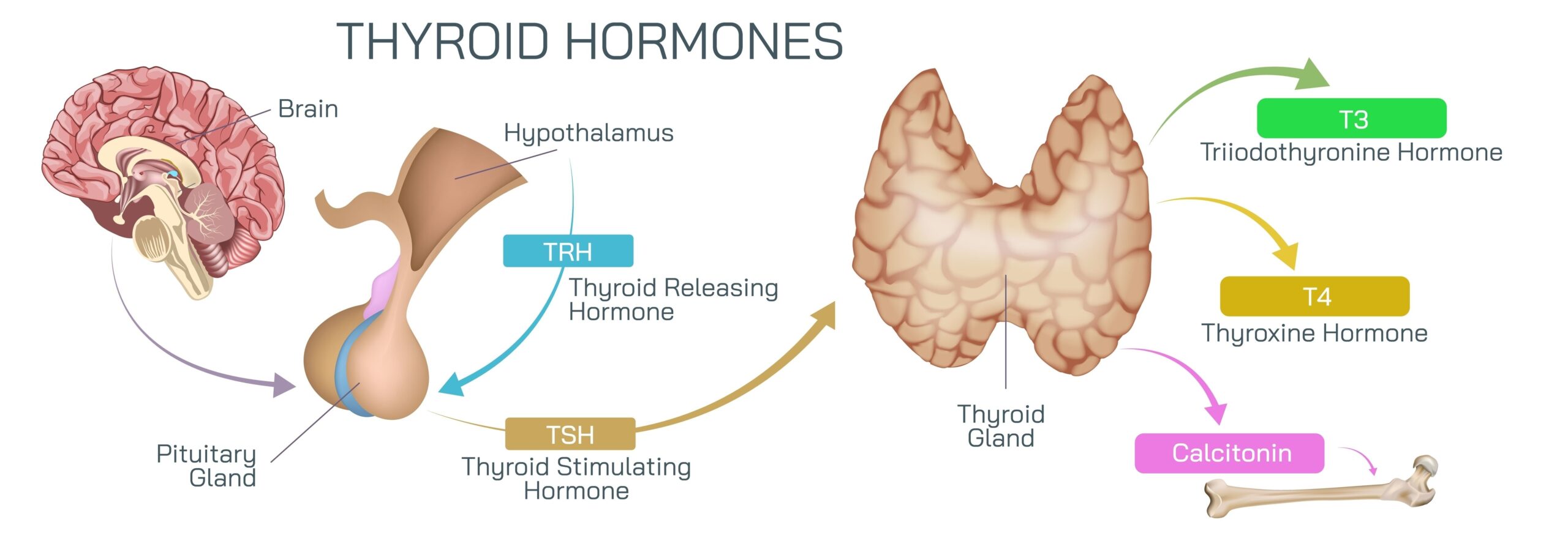
Your thyroid gland plays a crucial role in controlling your body’s metabolism by producing thyroid hormones—mainly thyroxine (T4) and triiodothyronine (T3). But how does your body know when to make more or less of these hormones? That’s where the feedback system comes in.
The hypothalamic-pituitary-thyroid axis
This system involves three key players:
- Hypothalamus: A part of your brain that acts like a thermostat. It senses the levels of thyroid hormones in your blood.
- Pituitary gland: A small gland just below the brain that responds to signals from the hypothalamus.
- Thyroid gland: The butterfly-shaped gland in your neck that produces thyroid hormones.
How the feedback loop works
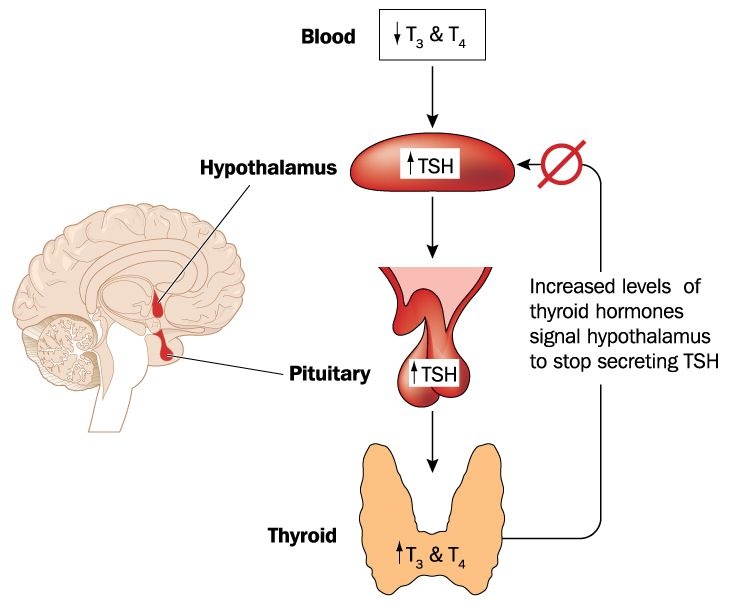
The hypothalamic-pituitary-thyroid axis works in the following way [10]:
- When your thyroid hormone levels (T3 and T4) in the blood are low, the hypothalamus releases a hormone called thyrotropin-releasing hormone (TRH).
- TRH signals the pituitary gland to release thyroid-stimulating hormone (TSH).
- TSH travels through your bloodstream to the thyroid gland, telling it to produce and release more T3 and T4.
- As the levels of thyroid hormones rise in your blood, they send a “stop” signal back to the hypothalamus and pituitary gland, reducing TRH and TSH production. This prevents your thyroid from making too much hormone.
- This loop keeps your thyroid hormone levels balanced, ensuring your metabolism stays steady.
Why this feedback system matters
If something disrupts this feedback loop, it can cause thyroid problems:
- Underactive thyroid (hypothyroidism): When the thyroid doesn’t produce enough hormones, TSH levels usually rise as the pituitary tries to stimulate it more [5].
- Overactive thyroid (hyperthyroidism): When the thyroid produces too much hormone, TSH levels usually drop because the pituitary senses there’s enough hormone already [7].
Doctors use blood tests measuring TSH and thyroid hormones to understand how well this feedback system is working and to diagnose thyroid conditions.
How is Hashimoto’s disease diagnosed?
Hashimoto’s disease, also known as Hashimoto’s thyroiditis, is an autoimmune condition where your immune system attacks your thyroid gland. This often leads to an underactive thyroid (hypothyroidism). Diagnosing Hashimoto’s involves a combination of your symptoms, blood tests, and sometimes imaging [5].
Symptoms and medical history
Your doctor will start by asking about your symptoms—such as tiredness, weight gain, feeling cold, constipation, and changes in your skin or hair. They’ll also ask about your family history, as thyroid problems can run in families.
Blood tests
The key to diagnosing Hashimoto’s is checking your thyroid function and looking for specific antibodies in your blood:
- Thyroid-stimulating hormone (TSH): Typically elevated if the thyroid isn’t producing enough hormones.
- Free thyroxine (free T4): Often low in Hashimoto’s.
- Free triiodothyronine (free T3): The active thyroid hormone. In early or mild Hashimoto’s, free T3 may remain normal as the body compensates by converting T4 to T3. In more advanced hypothyroidism, free T3 usually decreases.
- Reverse T3 (rT3): An inactive form of thyroid hormone. Measuring reverse T3 helps differentiate true hypothyroidism from other conditions affecting thyroid hormone metabolism. In Hashimoto’s, reverse T3 is usually normal or low. Using reverse T3 as a parameter to determine subclinical hypothyroidism remains a controversial topic [12].
- Thyroid peroxidase antibodies (TPOAb): Usually elevated in Hashimoto’s, indicating autoimmune attack on the thyroid.
- Thyroglobulin antibodies (TgAb): May also be raised but are less specific
Additional tests
Sometimes, a thyroid ultrasound may be done if there’s a lump or swelling in your neck. This can show if your thyroid gland is inflamed or has changed in size.
Summary:
Hashimoto’s disease is usually diagnosed by a combination of symptoms, high TSH, low T4, and raised thyroid antibodies—especially TPOAb.
How is Hashimoto’s disease treated?
Hashimoto’s disease is managed by replacing the thyroid hormones your body can no longer make in sufficient amounts. The main goal is to restore normal hormone levels, improve symptoms, and prevent long-term complications.
Standard treatment: Levothyroxine (T4)
- The usual treatment for Hashimoto’s is a daily tablet of levothyroxine, a synthetic form of thyroxine (T4) [12].
- Levothyroxine is converted in your body to the active hormone triiodothyronine (T3), which your cells need to function.
- Your doctor will start you on a low dose and adjust it based on regular blood tests (mainly TSH), symptoms, and your response.
Why T4-only therapy is the standard in the UK
- In the UK, the NHS and NICE guidelines recommend levothyroxine (T4) as the first-line—and usually only—treatment for underactive thyroid, including Hashimoto’s disease [12].
- This is because most people’s bodies can convert T4 to T3 naturally, and studies show that T4 alone works well for the vast majority of patients [13].
T4 and T3 combination therapy
- Some people with Hashimoto’s continue to feel tired, foggy, or unwell despite having “normal” blood test results on T4 alone.
- In other countries, a combination of T4 (levothyroxine) and T3 (liothyronine) may be prescribed for certain patients who don’t feel well on T4 alone.
- Research suggests that a small group of people may have trouble converting T4 to T3 efficiently, and these patients might benefit from combination therapy [14].
Why combination therapy isn’t usually offered in the UK
- In the UK, T3 (liothyronine) is not routinely recommended due to limited evidence of long-term benefit, concerns about side effects, and the high cost of T3 medication 13].
- The use of T3/T4 combination may be helpful in some people who do not get an adequate response from monotherapy of T4 [14].
Other important aspects of treatment
- Regular blood tests to monitor TSH and thyroid hormones are essential to ensure you’re on the correct dose.
- Some people may need adjustments to their medication over time, especially during pregnancy, illness, or with age.
- If you have other autoimmune conditions, your doctor will help you manage those too.
Summary:
Hashimoto’s disease is treated with levothyroxine (T4) in the UK. Although some people may benefit from a combination of T4 and T3, this is not routinely offered due to current guidelines and concerns about safety and evidence. If you continue to feel unwell on T4 alone, talk to your doctor about your options.
What are deiodinases?
Deiodinases are special enzymes that help your body fine-tune thyroid hormone activity right inside your cells. While your thyroid gland mainly releases thyroxine (T4), this hormone is not very active on its own. Deiodinases convert T4 into triiodothyronine (T3), the active form that your cells actually use, or into reverse T3 (rT3), an inactive form. This process lets different tissues adjust their own thyroid hormone levels, regardless of what’s happening in your bloodstream [15].
Types of deiodinases and where they work
Type 1 deiodinase (D1):
- Found mostly in the liver, kidneys, and thyroid gland.
- Converts T4 it to active T3.
- Responsible for much of the T3 circulating in your blood.
Type 2 deiodinase (D2):
- Located in the brain, pituitary gland, brown fat, and skeletal muscle.
- Converts T4 into T3 within local tissues, ensuring these areas get enough active hormone even if blood T3 is low.
- Plays a key role in regulating the feedback system that controls TSH release.
Type 3 deiodinase (D3):
- Found in the placenta, brain, and skin.
- Inactivates T4 and T3 by converting them into reverse T3 and T2, both inactive forms.
- Protects tissues from too much thyroid hormone.
How does deiodinase activity change with physiological conditions?
Deiodinase activity isn’t static—it changes in response to your body’s needs, illness, and other conditions [11], [15].:
- Illness or stress:
During severe illness, trauma, or starvation, D3 activity can increase, leading to an increase in reverse T3 and a decrease in active T3 in tissues. This is sometimes called “non-thyroidal illness syndrome” or “euthyroid sick syndrome.” The body does this to conserve energy during stress. - Pregnancy:
D3 activity rises in the placenta to protect the developing baby from too much thyroid hormone. - Inflammation:
Chronic inflammation can suppress D1 and D2 activity, thereby reducing T3 production in tissues and exacerbating symptoms of hypothyroidism, even when blood TSH and T4 levels are normal. - Ageing:
D1 activity may decrease with age, potentially leading to a decrease in circulating T3. - Genetic differences:
Some people have genetic variations that affect how well their deiodinases function, influencing their risk of symptoms despite “normal” blood test results.
Cellular hypothyroidism and why blood tests might miss it
Because deiodinases control thyroid hormone activity inside cells, it’s possible to have “cellular hypothyroidism”—where tissues aren’t getting enough T3—even if blood TSH and T4 are normal. For example:
- If D1 is low and D2 is high:
Blood T3 levels may drop, but the brain and pituitary (which utilise D2) still receive sufficient T3. TSH stays normal, masking tissue-level hypothyroidism elsewhere in the body. - If D3 is high:
More T4 is converted to inactive rT3, reducing the amount of active T3 available to cells. This can cause symptoms even if TSH is normal. - If D2 is low:
The brain and pituitary may sense a lack of T3 and respond by increasing TSH, even if other tissues are functioning correctly.
Why relying only on TSH can be problematic
- TSH reflects pituitary hormone status, not the whole body:
The pituitary is especially sensitive to local T3 through the D2 receptor. If D2 is functioning correctly in the brain but D1 is low elsewhere, TSH may be normal; however, other tissues can still be hypothyroid. - Symptoms can persist despite “normal” labs:
Patients may have fatigue, brain fog, or other hypothyroid symptoms even when TSH and T4 are in the normal range, because their tissues are starved of T3. - Treatment implications:
Standard treatment with levothyroxine (T4) relies on deiodinases to convert T4 to T3. If deiodinase activity is impaired (for example, low D1 or high D3), patients may not get enough T3 at the tissue level. These individuals might benefit from combination therapy with both T4 and T3, but this is not routinely offered in the UK.
Summary
Deiodinases are crucial for regulating the action of thyroid hormones within your cells. Their activity changes with illness, stress, age, pregnancy, and genetics. Because TSH mainly reflects pituitary thyroid status, relying on it alone can miss cellular hypothyroidism, where tissues aren’t getting enough T3. Understanding deiodinase activity can help guide more personalised thyroid treatment, especially for those who don’t feel better on standard therapy.
The role of Low Dose Naltrexone (LDN) in Hashimoto’s disease
Low Dose Naltrexone (LDN) is an emerging treatment that some people with autoimmune conditions, including Hashimoto’s thyroiditis, are exploring as a complementary therapy.
What is LDN?
LDN is a low-dose form of naltrexone, a medication traditionally used to treat addiction at much higher doses. At low doses, it is thought to modulate the immune system and reduce inflammation [16].
How might LDN help in Hashimoto’s?
Hashimoto’s is an autoimmune disease where the immune system mistakenly attacks the thyroid gland. LDN may help by:
- Regulating immune function to reduce the autoimmune attack on the thyroid.
- Lowering inflammation that contributes to symptoms.
- Potentially improving energy levels, mood, and overall well-being in some patients.
What does the research say?
Anecdotal evidence from numerous practitioners and patient reports suggests that Low Dose Naltrexone (LDN) may improve symptoms for some people living with Hashimoto’s. Many individuals and clinicians have shared positive experiences, noting improved energy, mood, and, in some cases, lower antibody levels.
The Norway study
This study used data from the Norwegian Prescription Database to examine whether starting low-dose naltrexone (LDN) affected thyroid hormone prescriptions in 898 patients with hypothyroidism. By comparing levothyroxine (LT4) and triiodothyronine (T3) dispensing one year before and after LDN initiation, the researchers found no significant changes in thyroid hormone use linked to LDN [17].
The study’s limitations
However, the study has significant limitations. It did not include any blood test results or clinical data, so it could not assess whether LDN influenced thyroid function or patient symptoms directly [17].
Prescription data alone may miss subtle improvements or worsening that do not lead to medication changes—additionally, the lack of patient symptom discussions and differentiation between types of hypothyroidism limits interpretation.
Without a control group and clinical context, it’s difficult to rule out confounding factors or fully evaluate LDN’s efficacy.
Given the positive responses LDN has shown in other autoimmune conditions and its excellent safety profile, it remains a potentially valuable option for patients who are not optimally managed on levothyroxine alone. More rigorous clinical trials with symptom and thyroid function monitoring are needed to clarify its role in hypothyroidism.
Is LDN a replacement for standard treatment?
No. LDN is not a substitute for thyroid hormone replacement therapy (levothyroxine) or other standard treatments.
LDN safety and side effects
LDN is generally well tolerated at low doses, with few reported side effects. Common mild side effects may include vivid dreams or sleep disturbances, which often improve over time.
LDN Summary
While not yet a mainstream treatment, LDN offers hope for some people with Hashimoto’s looking to manage their autoimmune symptoms alongside conventional care.
If you’re interested in LDN, complete the online consultation to see if LDN is safe for you or contact us for further information. Selenium and Hashimoto’s thyroiditis: What does the research say?
Selenium and Hashimoto’s disease
Hashimoto’s thyroiditis (HT) is a common cause of an underactive thyroid. Selenium is a mineral essential for making thyroid hormones and protecting the thyroid gland from damage.
Researchers reviewed numerous studies to determine if taking selenium supplements benefits individuals with HT. They examined the impact of selenium on thyroid hormone levels, thyroid antibodies (which indicate the extent of immune system attack on the thyroid), ultrasound scans of the thyroid, immune system markers, patient symptoms, and any side effects [18].
What they found:
- Selenium supplements helped lower thyroid-stimulating hormone (TSH) levels in people with HT who were not yet on thyroid hormone replacement therapy. Lower TSH usually indicates that the thyroid is functioning more effectively [18].
- Selenium also reduced levels of thyroid peroxidase antibodies (TPOAb), which are involved in the autoimmune attack on the thyroid [18].
- Markers of oxidative stress (damage caused by harmful molecules) also decreased with selenium [18].
- There were no significant changes in other thyroid hormones (T3, T4) or thyroid size [18].
- Selenium was safe, with no more side effects than a placebo [18].
What does this mean?
Taking selenium may help improve thyroid function and reduce autoimmune activity in people with Hashimoto’s, especially if they are not yet on thyroid hormone treatment. However, the evidence isn’t perfect, and more research is needed.
Important notes:
- Selenium levels vary by diet and region, so that some people may benefit more than others.
- Too much selenium can be harmful, so supplements should be taken carefully and under medical advice.
- More large, high-quality studies are needed to confirm these findings and to understand who benefits most.
This information is for general guidance only. For medical advice, please consult your doctor or healthcare provider.
Reference:
- NHS (2024) Underactive thyroid (hypothyroidism). [Online] NHS. Available at: https://www.nhs.uk/conditions/underactive-thyroid-hypothyroidism/ (Accessed: 27 September 2025).
- Wro?ska, K., Ha?asa, M. and Szczuko, M., 2024. The role of the immune system in the course of Hashimoto’s Thyroiditis: the current state of knowledge. International Journal of Molecular Sciences, 25(13), p.6883.
- Kristensen, B. and Hegedüs, L., 2016. Regulatory B and T cell responses in patients with autoimmune thyroid disease and healthy controls. Danish medical journal, 63(2), p.B5177.
- Salman, A.G., Mahdi, I.A.J., Mukhlef, A.K., abd alsattar Mohammad, R., Zaghir, M.S.H. and muatez Wadaa’a, N., 2024. Physiological aspects of thyroid disorders: Anatomy, hormones, diagnosis and management. Current Clinical and Medical Education, 2(05), pp.17-32.
- Wilson, S.A., Stem, L.A. and Bruehlman, R.D., 2021. Hypothyroidism: diagnosis and treatment. American family physician, 103(10), pp.605-613.
- Kasumagic-Halilovic, E., 2014. Thyroid disease and the skin. Annals Thyroid Res, 1(2), pp.27-31.
- Kravets, I., 2016. Hyperthyroidism: diagnosis and treatment. American family physician, 93(5), pp.363-370.
- NHS (2024) Overactive thyroid (hyperthyroidism). [Online] NHS. Available at: https://www.nhs.uk/conditions/overactive-thyroid-hyperthyroidism/ (Accessed: 27 September 2025).
- Novodvorsky, P. and Allahabadia, A., 2017. Thyrotoxicosis. Medicine, 45(8), pp.510-516.
- Chiamolera, M.I. and Wondisford, F.E., 2009. Thyrotropin-releasing hormone and the thyroid hormone feedback mechanism. Endocrinology, 150(3), pp.1091-1096.
- Gomes-Lima, C., Wartofsky, L. and Burman, K., 2019. Can reverse T3 assay be employed to guide T4 vs. T4/T3 therapy in hypothyroidism?. Frontiers in Endocrinology, 10, p.856.
- CKS (2025) Overt hypothyroidism – non-pregnant: management. [Online] NICE Clinical Knowledge Summaries. Available at: https://cks.nice.org.uk/topics/hypothyroidism/management/overt-hypothyroidism-non-pregnant/ (Accessed: 27 September 2025).
- Ahluwalia, R., Baldeweg, S.E., Boelaert, K., Chatterjee, K., Dayan, C., Okosieme, O., Priestley, J., Taylor, P., Vaidya, B., Zammitt, N. and Pearce, S.H., 2023. Use of liothyronine (T3) in hypothyroidism: Joint British Thyroid Association/Society for endocrinology consensus statement. Clinical Endocrinology, 99(2), pp.206-216.
- Dayan, C. and Panicker, V., 2018. Management of hypothyroidism with combination thyroxine (T4) and triiodothyronine (T3) hormone replacement in clinical practice: a review of suggested guidance. Thyroid research, 11(1), p.1.
- Sabatino, L., Vassalle, C., Del Seppia, C. and Iervasi, G., 2021. Deiodinases and the three types of thyroid hormone deiodination reactions. Endocrinology and Metabolism, 36(5), pp.952-964.
- Courier Pharmacy (2025) How does LDN work? [Online] Courier Pharmacy. Available at: https://courierpharmacy.co.uk/how-does-ldn-work/ (Accessed: 27 September 2025).
- Raknes, G. and Småbrekke, L., 2020. No change in the consumption of thyroid hormones after starting low dose naltrexone (LDN): a quasi-experimental before-after study. BMC endocrine disorders, 20(1), p.151.
- Huwiler, V.V., Maissen-Abgottspon, S., Stanga, Z., Mühlebach, S., Trepp, R., Bally, L. and Bano, A., 2024. Selenium supplementation in patients with Hashimoto thyroiditis: a systematic review and meta-analysis of randomized clinical trials. Thyroid, 34(3), pp.295-313.
BSc Pharmacy, Independent Prescriber, PgDip Endocrinology, MSc Endocrinology, PgDip Infectious Diseases
Superintendant Pharmacist, Independent Prescriber
BSc Pharmacy
Compounding Pharmacist

