





What you should know about female hair loss
Shedding some hair daily is completely normal, and noticeable thinning is very common too, especially with age and hormonal change. As the NHS explains, female hair loss is usually not a sign of anything serious. It’s still worth getting checked, partly to find the cause and partly to rule out treatable issues like low iron or a thyroid problem.
Female pattern hair loss is the most common cause. As the dermatology literature describes, it involves follicles gradually shrinking and producing finer hair, often influenced by genetics and hormones. Other causes include temporary shedding after stress or illness, thyroid problems, and iron deficiency, which is why a proper diagnosis matters.
To help prevent acne, maintain a skincare routine that includes gentle cleansing, avoid touching your face, use non-comedogenic products, and manage stress. Eating a balanced diet and staying hydrated can also help.
For female pattern hair loss, topical minoxidil is the proven starting point. It takes around four months to work and needs to be continued. Other treatments may be added depending on your type of hair loss, your biology, and how you respond.
Gro is Courier Pharmacy’s compounded hair loss range. It offers minoxidil, tretinoin, and the anti-androgens finasteride and dutasteride, alone or in combination, in a choice of liquid, foam, or gentle alcohol-free Trichosol base. Each 30ml bottle lasts about a month and costs £29.99, under £1 a day. Everything is prescription-only and assessed first.
Sometimes, but with care. These anti-androgen treatments can help certain women, and are more often used after the menopause. The crucial point is pregnancy. You must not use them, or tretinoin, if you are pregnant or could become pregnant, as they can harm a developing baby. Pre-menopausal women need reliable contraception, and a prescriber will assess suitability first.
TrichoTest is a pharmacogenetic test that analyses 26 genetic markers across nine pathways linked to hair loss and how you respond to treatment. Combined with your medical history, it helps your prescriber choose the ingredients and doses most likely to suit you, rather than relying on trial and error. We offer it alongside a full pharmacist consultation. It guides treatment, but doesn’t guarantee results.
Often, yes. We can review what you’ve tried, check for underlying causes with blood tests, use TrichoTest to personalise your plan, and offer compounded Gro options when standard products don’t suit. It starts with a free chat with one of our pharmacists.
Additional information
Female hair loss
Female hair loss can creep up quietly, a wider parting here, more strands in the plughole there, until one day it’s all you can see in the mirror. If your hair feels thinner than it used to, you’re far from alone, and you’re far from out of options. At Courier Pharmacy, we believe healthcare should fit the person, not force the person to fit the system. So we build support around your hair, your hormones, and your goals, with treatment tailored to you, honest guidance from real pharmacists, a community that gets it, and care you can trust. Hair loss treatment that fits you, the way it should be. Noticing more hair in the brush than on your head? We can help you manage female hair loss.

Five key takeaways
- Female hair loss is common and rarely talked about. As the NHS notes, many women experience thinning hair at some point, especially with age and hormonal change.
- It comes in different forms. The most common is female pattern hair loss, but stress, illness, thyroid problems, and iron deficiency can all play a part, as NICE Clinical Knowledge Summaries describe.
- The right diagnosis changes everything. Treatments that help one type of hair loss may do nothing for another, so identifying the cause comes first.
- Topical minoxidil is the proven starting point. As the Cochrane review by van Zuuren and colleagues found, it’s the best-evidenced treatment for female pattern hair loss.
- Personalised beats generic. Compounded options, genetic testing, and the right combination of ingredients can succeed where one-size-fits-all products fall flat.

What Courier Pharmacy offers for female hair loss
- Topical minoxidil and other evidence-based hair loss treatments
- TrichoTest, a pharmacogenetic test that helps personalise your treatment plan
- The Gro range, our compounded hair loss line created with Medical Mojo, in liquid, foam, or gentle alcohol-free and propylene glycol-free bases
- Personalised compounded formulations tailored to your scalp, with women-focused options in development
- Blood tests to check for underlying causes like low iron, thyroid issues, or hormonal imbalance
- Prescription options, where appropriate, with full pharmacist guidance on benefits and risks
- Free fortnightly drop-in clinics in Derby, with no cost and no pressure

What you should know about female hair loss treatments
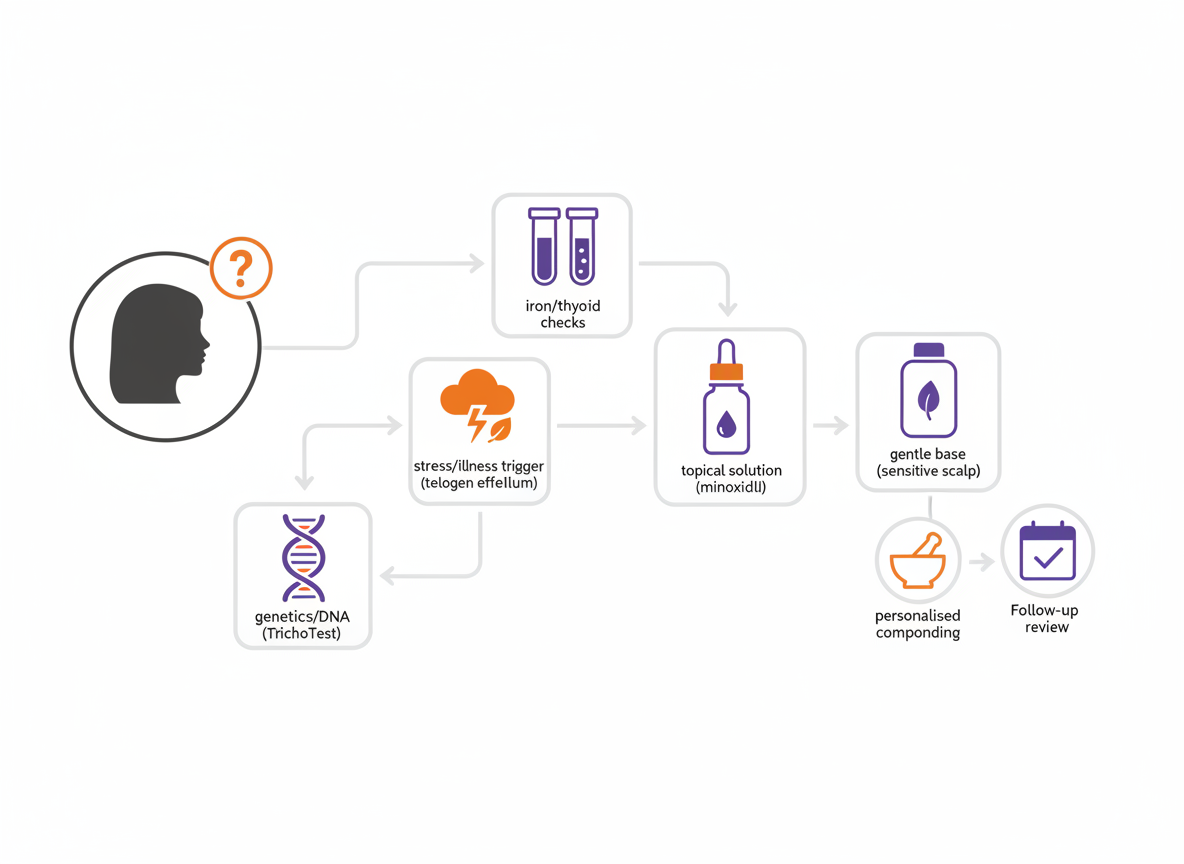
Good female hair loss care follows a clear, sensible path. First, get the right diagnosis, because not all hair loss is the same. Second, look for any reversible cause, like low iron or a thyroid problem. Third, use treatments that genuinely have evidence behind them, starting with topical minoxidil. Fourth, tailor that plan to you and review it as your hair responds.
This is the approach we lean on at Courier Pharmacy. As our own review of female hair loss explains, the most successful plans are personal ones, built around your biology, your routine, and what you’re hoping to achieve. The goal isn’t someone else’s hair. It’s hair you feel like yourself in.
Female hair loss overview
Female hair loss is any noticeable thinning or shedding of hair in women, from a widening parting to diffuse loss across the scalp. The NHS describes hair loss as common and usually not a sign of anything serious, though it can be deeply upsetting.
The emotional impact is real and often underestimated. Hair is tied up with identity and confidence, so losing it can affect mood, relationships, and how you feel walking into a room. None of that is vanity, and none of it is something you simply have to accept in silence.
The treatment landscape is more hopeful than many women realise. As the peer-reviewed review by Ho and colleagues on pattern hair loss explains, several effective options exist, and combining them often works better than relying on one. The key is matching the treatment to the type of hair loss, which is why a proper assessment matters so much.
Why does all this matter? Because female hair loss is common, frequently treatable, and too often dismissed. Many women are told it’s “just hormones” and sent away. You deserve a proper look and a plan that fits, not a shrug.

What is female hair loss?
Female hair loss covers several conditions, but the most common is female pattern hair loss, also called female androgenetic alopecia. As the dermatology literature explains, this is a gradual thinning where hair follicles shrink over time and produce finer, shorter hairs.
Common signs include:
- A widening centre parting
- Thinning over the crown and top of the scalp
- Hair that feels finer, flatter, or harder to style
- More shedding than usual, on the pillow, brush, or shower floor
- A ponytail that feels noticeably thinner
- In some cases, patchy loss rather than diffuse thinning
Unlike men, women usually keep their frontal hairline in female pattern hair loss. As the literature notes, the thinning tends to spread out across the top rather than receding at the temples.

How common is female hair loss?
Female hair loss is far more common than its hushed reputation suggests. The dermatology literature reports that female pattern hair loss affects a large proportion of women, with prevalence rising steadily with age and rising sharply after the menopause.
Some studies suggest female pattern hair loss affects up to half of women over the age of 50, as the systematic review on spironolactone by Wang and colleagues notes. Other forms of hair loss are common too. Alopecia areata, an autoimmune condition, affects around 2% of people at some point in their lives, and temporary shedding after stress or childbirth is something many women experience. In short, you are in very large company.
What causes female hair loss?
There’s often more than one cause at play. Female hair loss can stem from genetics, hormones, health, and lifestyle, sometimes in combination. The NHS and NICE Clinical Knowledge Summaries describe several recognised contributors.
Genetic and hormonal factors
Female pattern hair loss runs in families and is linked to how sensitive your follicles are to androgens, a group of hormones that includes testosterone. As the dermatology literature explains, this sensitivity gradually shrinks the follicles, especially after the menopause.
Telogen effluvium
This is temporary shedding triggered by a shock to the system, such as childbirth, severe illness, surgery, crash dieting, or major stress. As NICE Clinical Knowledge Summaries note, it usually settles on its own within six to twelve months once the trigger passes.
Autoimmune causes
In alopecia areata, the immune system mistakenly attacks hair follicles, causing patchy loss. It can come and go, and sometimes regrows on its own. This type needs a different approach from pattern hair loss.
Nutritional and medical causes
Low iron, thyroid problems, and conditions like polycystic ovary syndrome can all cause or worsen hair loss. As the NHS notes, treating the underlying issue can itself help hair recover, which is why testing matters.
Hairstyling and traction
Tight ponytails, braids, extensions, and some chemical treatments can pull on the hair and cause traction alopecia over time. Caught early, this is often reversible.
Medication-related causes
Some medicines list hair loss as a side effect. If you’ve noticed shedding after starting something new, it’s worth a chat with a pharmacist rather than stopping anything yourself.
What happens in the body with female hair loss?
Every hair on your head follows a cycle. It grows for a few years, rests briefly, then sheds so a new hair can take its place. As the dermatology literature describes, at any moment most of your hair is in the growing phase, which is why a little daily shedding is completely normal.
In female pattern hair loss, this cycle shifts. The growing phase gets shorter, and affected follicles gradually shrink in a process called miniaturisation. Each new hair grows back a little finer and shorter than the last, until some follicles stop producing visible hair at all. The hormone dihydrotestosterone, or DHT, plays a key role in follicles that are genetically sensitive to it.
In telogen effluvium, something different happens. A stressor pushes many hairs into the resting phase at once, so they shed together a few months later. This explains the alarming “handfuls” some women notice after childbirth or illness, and why it usually recovers.

Diagnosing female hair loss
Getting the diagnosis right is the most important step, and it usually starts with a conversation, not a test. A clinician will ask about your pattern of loss, family history, recent health, stress, diet, and medicines, then examine your scalp. As NICE Clinical Knowledge Summaries advise, this clinical picture often points to the cause.
A close look at the scalp and hair, sometimes with a dermoscope, helps tell the different types apart. Blood tests aren’t always needed, but they’re useful for spotting reversible causes such as iron deficiency, thyroid problems, or hormonal imbalance.
This is one area where Courier Pharmacy can help directly. We can arrange blood panels covering things like ferritin, thyroid function, and vitamin D, so nothing treatable gets missed. We also offer TrichoTest, a genetic test that looks at the factors influencing your hair loss to help personalise your plan. Tests that answer the question, not just tick a box.
Managing female hair loss: current treatments
The modern approach is practical and increasingly personalised. As the peer-reviewed review by Ho and colleagues explains, the best results often come from combining treatments and sticking with them. The order of play usually starts simply, then builds.
First, treat anything reversible. If low iron, a thyroid problem, or another condition is contributing, addressing it can make a real difference on its own, as the NHS notes. Second, start the best-evidenced treatment, which for female pattern hair loss is topical minoxidil. Third, where minoxidil alone isn’t enough, your prescriber may add or combine other ingredients, and this is where personalised compounding earns its keep. Throughout, patience matters, because most treatments need several months before you can judge them, and many need to be continued to hold their gains.
The active ingredients we use for female hair loss
No single ingredient suits everyone, which is exactly why we tailor. Here’s a plain-English tour of the actives most relevant to female hair loss, what they do, and where they fit.
Minoxidil
Minoxidil is the proven starting point. As the Cochrane review by van Zuuren and colleagues found, topical minoxidil is the best-evidenced treatment for female pattern hair loss. It supports the active growth phase of the hair cycle. Interestingly, it’s a pro-drug, meaning your scalp has to switch it on using an enzyme called SULT1A1, and as the review by Suchonwanit and colleagues explains, people vary in how well they do that. That’s why it works brilliantly for some and modestly for others. It takes around four months to show results and needs to be continued to maintain them. A low-dose oral version is also growing in popularity, used off-label and only after assessment.
Finasteride and dutasteride
These are anti-androgens, better known for male hair loss, that reduce the DHT driving follicle shrinkage. Finasteride blocks one form of the enzyme involved, while dutasteride blocks two, so it acts a little more broadly. In women they’re used off-label, usually after the menopause, and they can be compounded as topical solutions to lower the amount absorbed. There’s one firm rule: they must never be used in pregnancy, which we’ll come back to below.
Tretinoin
Tretinoin is a vitamin A derivative often added in small amounts to help the other ingredients work better. It can improve how well minoxidil is absorbed and activated, which may help women who haven’t responded to minoxidil alone. It can also increase sensitivity and sun sensitivity, so it’s used carefully and at low strength.
Spironolactone
Spironolactone is an oral anti-androgen that some women take, particularly those with signs of hormonal imbalance such as polycystic ovary syndrome. As the systematic review by Wang and colleagues describes, it can help, often working best alongside minoxidil. It’s prescribed off-label, and like the other anti-androgens, it carries a clear pregnancy caution and needs reliable contraception in women who could conceive.
17?-oestradiol (topical oestrogen)
Topical oestrogen, usually in the form of 17?-oestradiol, also called alfatradiol, is used in some countries for female pattern hair loss. It’s a non-feminising form of oestrogen, so it acts on the scalp without the body-wide effects of standard oestrogen. The dermatology literature suggests it may influence how follicles respond to androgens locally, though the evidence is more modest than for minoxidil. It’s a women-specific option, and one we pair with minoxidil in our compounded Gro formulations for women. As with any hormone treatment, it’s prescription-only and assessed individually.
Cetirizine
You may know cetirizine as a hay-fever tablet, but topical cetirizine is an intriguing newer option for hair loss. Balding scalps tend to have raised levels of a molecule called prostaglandin D2, which holds hair growth back. Cetirizine helps lower it. In a randomised study of women with female pattern hair loss, topical cetirizine added to minoxidil improved results, and it’s generally well tolerated. That makes it a useful, non-hormonal choice, especially for women who can’t get on with minoxidil alone.
Supplements: biotin and Nourkrin
Biotin, or vitamin B7, is the most heavily marketed hair supplement of all. The honest picture is that it mainly helps when there’s a genuine deficiency, which is uncommon on a normal diet. As a 2024 review in the Journal of Clinical and Aesthetic Dermatology concluded, there’s little evidence it benefits people who aren’t deficient. It can also interfere with some blood tests, including thyroid tests, so it’s worth telling your clinician if you take it.
Nourkrin is a different kind of supplement. It’s an oral proteoglycan replacement therapy, built around a marine complex called Marilex, designed to support the hair growth cycle from the inside. As the research on proteoglycan replacement therapy describes, studies in women with female pattern hair loss and diffuse shedding have reported improved hair count and satisfaction over several months. Much of that evidence is open-label and industry-linked, so we’d frame Nourkrin as a promising add-on rather than a certainty. It’s taken daily for at least six months to judge, and isn’t suitable if you have a fish or shellfish allergy. As always, we’d rather test first and recommend supplements only where they’re likely to help.

The Gro range: compounded hair loss treatment that fits you
Off-the-shelf products don’t suit everyone. Some women need a particular strength, others need a combination, and many need a base that won’t irritate a sensitive scalp. This is where Courier Pharmacy’s personalised compounding comes in. Compounding simply means a medicine made to order for one person by a licensed pharmacy, shaped around you rather than the other way round.
Our compounded hair loss line is called Gro, created by Courier Pharmacy and our partners at Medical Mojo, who handle the education while we handle the treatment. The active ingredients used across the range include minoxidil, tretinoin, and the anti-androgens finasteride and dutasteride, prescribed alone or in combination at the concentration chosen for you. Gro comes in three formats: a traditional topical liquid, a lighter foam, and a Trichosol solution that is completely free from alcohol and propylene glycol, the two most common causes of scalp stinging and dryness.
That last detail matters more than it sounds, because a treatment only works if you keep using it. For reactive scalps, a gentler base can be the difference between sticking with it and quietly giving up. Each Gro option comes as a 30ml bottle that lasts around a month, for £29.99, which works out at less than £1 a day.
Many of the established Gro combinations were developed with men’s pattern hair loss in mind, since finasteride and dutasteride are used more freely in men. We’re now extending the range with combinations designed specifically for women with female hair loss. A good example is 17?-oestradiol paired with minoxidil, a women-focused formula that combines a non-feminising scalp oestrogen with the best-evidenced growth treatment. Other tailored options pair minoxidil with actives like tretinoin or cetirizine. As with everything we compound, these are prescription-only and supplied only after a proper clinical assessment, so the formula and strength are right for you.

An important safety note for women who could become pregnant
Some hair loss treatments work by lowering or blocking androgens, the hormones that drive pattern thinning. This group includes the anti-androgen spironolactone and the DHT-blocking medicines finasteride and dutasteride. They can genuinely help some women, but they carry one firm rule. You must not use them if you are pregnant, trying to conceive, or might become pregnant, because they can interfere with the healthy development of a baby, particularly a male baby.
Tretinoin needs the same caution. As a vitamin A based retinoid, it’s best avoided in pregnancy and while breastfeeding, even as a topical, because retinoids are linked to risks in pregnancy. Oestrogen-based options carry their own cautions too.
So if you are pre-menopausal and considering any of these treatments, reliable contraception is essential throughout, and you should stop and speak to your prescriber straight away if you think you might be pregnant. This is exactly why these medicines are prescription-only, and why we assess every person individually before supplying them. If you’d like to talk it through, our pharmacists are here to help you weigh it up honestly.
TrichoTest: hair loss treatment matched to your genetics
One of the hardest things about hair loss is the trial and error. You commit to a treatment, wait months to see if it works, and start again if it doesn’t. TrichoTest is designed to cut through that, and it’s one of the tools we’re proudest to offer.

What TrichoTest does
TrichoTest is a simple cheek-swab pharmacogenetic test. It analyses 26 genetic markers linked to nine pathways involved in hair loss and how you respond to treatment, then combines your genetic profile with your medical history and lifestyle. From that, it predicts which ingredients, doses, and delivery methods are most likely to suit your biology. In practice, it looks at areas including:
- How well you process minoxidil and related growth treatments
- How effectively you respond to anti-androgen medicines like finasteride and dutasteride
- Your circulation, collagen, and growth-factor responses
- How you absorb key vitamins and minerals, and your antioxidant needs
Why it’s useful
Instead of guessing, your prescriber starts with a plan shaped around your genetics. That can mean choosing the right active from the outset, spotting when a standard treatment is unlikely to work for you, or picking up nutritional gaps worth addressing alongside treatment. For a compounded range like Gro, that’s especially powerful, because we can build your formula around what your results suggest.
TrichoTest doesn’t guarantee results, and it never replaces a clinical assessment. What it does is give you and your prescriber better information, so you spend less time and money on things that were never likely to help, and more on what is.

Finding the root cause: blood tests and the DUTCH test
Female hair loss rarely has a single, obvious cause, and treating it well means finding out what’s actually driving it. Alongside TrichoTest, which looks at your genetics, two more tools help us get to the root: blood tests and the DUTCH hormone test. Together they turn guesswork into a plan.
Blood tests
A simple blood panel can reveal several of the most common, and most treatable, causes of hair loss. As the NHS notes, correcting an underlying issue can sometimes improve your hair on its own. We can arrange tests that check:
- Iron and ferritin, since low iron is a frequent cause of shedding in women
- Thyroid function, as both an underactive and overactive thyroid affect hair
- Vitamin D and B12, which support healthy hair growth
- Hormone markers such as testosterone, free testosterone, and DHEA, which can flag androgen excess or conditions like polycystic ovary syndrome
The DUTCH test
The DUTCH test, which stands for Dried Urine Test for Comprehensive Hormones, goes a step further. It’s a functional hormone test that uses dried urine samples collected across a day. Its real strength is that it shows not just how much of a hormone you have, but how your body is processing it, which a single blood reading can miss.
For hair loss, the most useful part is what it reveals about your androgens. As the hormone-testing literature describes, the DUTCH test maps whether your body is sending testosterone down the potent DHT pathway, driven by an enzyme called 5-alpha-reductase. It reads this through DHT’s metabolites, such as 5-alpha-androstanediol and androsterone. Because DHT is the main hormonal driver of female pattern hair loss, an overactive DHT pathway can be a genuine root cause, and one that standard blood tests don’t always pick up. The test also measures cortisol, your main stress hormone, which is linked to shedding, along with your oestrogen and progesterone balance.

Why this matters
Knowing your hormonal picture helps target treatment rather than guess at it. If your DHT pathway is running high, that points towards anti-androgen or DHT-focused approaches, and even nutrients like zinc that influence 5-alpha-reductase. If stress and cortisol are the bigger driver, the plan looks different. It’s the same idea behind everything we do: understand your biology first, then build the treatment around it.
The DUTCH test is a private, functional test that complements standard care rather than replacing it, and its results need expert interpretation. That’s exactly what our team offers. We can arrange blood tests and the DUTCH test, read them together with your TrichoTest and history, and shape a plan that fits you. Tests that answer the question, not just tick a box.

Patient experiences and challenges
If you’ve ever been told your hair loss is “just hormones” or “nothing to worry about,” you’ll know how dismissive that feels. It’s one of the most common frustrations women share with us. The distress is real, even when others can’t yet see the thinning.
Many women also tell us they suffered in silence, assuming nothing could be done, or felt embarrassed to bring it up at all. Others spent money on products with no evidence, or gave up on a treatment just before it would have worked. As our own review of female hair loss highlights, knowing what genuinely helps, and how long to give it, makes all the difference.
Here’s what we want you to hear. You’re not vain, and you’re not overreacting. You’re not broken either. Female hair loss is real, common, and often treatable, and the problem has usually been the one-size-fits-all system, not you. You’re the one living in your skin, and you get to decide what feeling like yourself looks like. Our job is simply to guide you there.
Innovative and new treatments for female hair loss
Female hair loss care is moving forward, and several newer options are worth knowing about. As always, we’d weigh the evidence rather than the hype.
Personalised, genetic-led care is one of the most exciting shifts, and it’s where our TrichoTest service comes in, matching treatment to your genetics rather than relying on trial and error, as covered in its own section above.
Beyond testing, topical cetirizine is an interesting non-hormonal newcomer, with a randomised study showing benefit in female pattern hair loss when added to minoxidil. Low-dose oral minoxidil has also gained ground, and platelet-rich plasma and low-level laser therapy are under active study. For alopecia areata specifically, newer medicines called JAK inhibitors have been approved for severe cases, as recent NICE technology appraisals describe. These are specialist treatments, not first steps.
Looking to the future: research and hope
The direction of travel is encouraging. Researchers are refining who benefits from which treatment, developing better-targeted medicines, and using genetic insights to personalise care from the start. The peer-reviewed literature points to a future where hair loss treatment is far less one-size-fits-all.
There’s reason for steady optimism. Female hair loss is one of the most actively researched areas in dermatology, and our understanding keeps deepening. We won’t promise miracles or overnight regrowth. What we will say is that more women are getting real results than ever before, and the right plan can help you hold on to your hair and your confidence.
How Courier Pharmacy helps with female hair loss
We started Courier Pharmacy because too many people get one-size-fits-all care and a closed door. Female hair loss is a perfect example. Your hair, your hormones, and your goals are unique, so your plan should be too. That personalisation is the first of our four pillars, and it’s why we offer tools like TrichoTest and the compounded Gro range.
The other three pillars carry it the rest of the way. Guidance means real pharmacists who help you understand your options, weigh the benefits and risks, and avoid wasting time or money on things that won’t help. Trust means we’re a UK-regulated pharmacy, transparent about what the evidence supports and what it doesn’t, working from NHS, NICE and peer-reviewed sources. Community means we show up for people even when there’s nothing to buy.
That spirit has a face in Dr Ada Jex-Cori, the voice of our approach, whose message is simple: you’re not broken, the system is, and we’re here to change that. It’s hair loss treatment that fits you, from a team that would rather earn your trust than sell you a quick fix.
Frequently asked questions about female hair loss

Is female hair loss serious?
Usually not. As the NHS explains, most female hair loss is caused by common things like ageing, hormonal change, and conditions such as female pattern hair loss, and isn’t dangerous. It’s still worth getting checked, partly to find the cause and partly to rule out treatable issues like low iron or a thyroid problem.
What’s the best treatment for female hair loss?
For female pattern hair loss, topical minoxidil is the proven starting point. The Cochrane review by van Zuuren and colleagues found it to be the best-evidenced option. It takes around four months to work and needs to be continued. Other treatments may be added depending on your type of hair loss, your biology, and how you respond.
What is the Gro range?
Gro is Courier Pharmacy’s compounded hair loss range, created with Medical Mojo. It offers minoxidil, tretinoin, and the anti-androgens finasteride and dutasteride, alone or in combination, in a choice of liquid, foam, or gentle alcohol-free Trichosol base. Each 30ml bottle lasts about a month and costs £29.99, under £1 a day. Everything is prescription-only and assessed first.
Can women take finasteride, dutasteride, or spironolactone for hair loss?
Sometimes, but with care. These anti-androgen treatments can help certain women, and are more often used after the menopause. The crucial point is pregnancy. You must not use them if you are pregnant or could become pregnant, as they can harm a developing baby. Pre-menopausal women need reliable contraception, and a prescriber will assess suitability first.
What is TrichoTest?
TrichoTest is a pharmacogenetic test that analyses 26 genetic markers across nine pathways linked to hair loss and how you respond to treatment. Combined with your medical history, it helps your prescriber choose the ingredients and doses most likely to suit you, rather than relying on trial and error. We offer it alongside a full pharmacist consultation. It guides treatment, but doesn’t guarantee results.
Does biotin help with hair loss?
Only sometimes. As a 2024 review in the Journal of Clinical and Aesthetic Dermatology concluded, biotin mainly helps when there’s a genuine deficiency, which is uncommon on a normal diet, and there’s little evidence it benefits people who aren’t deficient. It can also interfere with some blood tests. We’d rather test first and supplement only where it’s likely to help.
What if I can’t use minoxidil?
You have options. Some women don’t tolerate minoxidil or don’t respond well to it. Alternatives and add-ons include topical cetirizine, a non-hormonal treatment shown to help female pattern hair loss in a randomised study, along with anti-androgens, oestradiol-based compounds, and treating any underlying cause. A prescriber can help you find a route that suits you.
Can Courier Pharmacy help if I’ve tried things that didn’t work?
Often, yes. We can review what you’ve tried, check for underlying causes with blood tests, use TrichoTest to personalise your plan, and offer compounded Gro options when standard products don’t suit. It starts with a free chat with one of our pharmacists.
More than a condition: our community
Living with hair loss can feel isolating, especially when people assume it’s trivial or purely cosmetic. So we made a space where it isn’t. Every fortnight, we run free drop-in clinics and talks at Insomnia in Derby, from 10 to 12pm. No cost. No pressure. Just real support, honest answers, and people who understand.
How this content was created
Written by the Courier Pharmacy editorial team and reviewed by a GPhC-registered pharmacist. Grounded in the latest NHS, NICE, BNF and EMC guidance, peer-reviewed studies, and the real questions patients bring to our drop-in clinics in Derby.
By the Courier Pharmacy editorial team. Medically reviewed by a GPhC-registered pharmacist. Last reviewed: June 2026.
Important disclaimer
This page is for general information and education. It isn’t medical advice, and it isn’t a substitute for a consultation with a qualified healthcare professional. The treatments mentioned, including compounded medicines, anti-androgens, and oestrogen-based options, are prescription-only and may not be suitable for you. Some carry serious risks in pregnancy. Always speak to a prescriber or pharmacist before starting, stopping, or changing any treatment, and never use a prescription medicine that wasn’t prescribed for you.
References
[1] National Health Service (2024) Hair loss. Available at: https://www.nhs.uk/conditions/hair-loss/ (Accessed: 22 June 2026).
[2] National Institute for Health and Care Excellence (no date) Alopecia, androgenetic: Clinical Knowledge Summary. Available at: https://cks.nice.org.uk/topics/alopecia-androgenetic/ (Accessed: 22 June 2026).
[3] National Institute for Health and Care Excellence (2023) Alopecia areata: Clinical Knowledge Summary. Available at: https://cks.nice.org.uk/topics/alopecia-areata/ (Accessed: 22 June 2026).
[4] van Zuuren, E.J., Fedorowicz, Z., Carter, B. and Pijl, S. (2016) ‘Interventions for female pattern hair loss’, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.CD007628.pub4. Available at: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD007628.pub4/full (Accessed: 22 June 2026).
[5] Suchonwanit, P., Thammarucha, S. and Leerunyakul, K. (2019) ‘Minoxidil and its use in hair disorders: a review’, Drug Design, Development and Therapy. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6691938/ (Accessed: 22 June 2026).
[6] Wang, C., Du, Y., Bi, L., Wang, X. and Zhao, Y. (2023) ‘The Efficacy and Safety of Oral Spironolactone in the Treatment of Female Pattern Hair Loss: A Systematic Review and Meta-Analysis’, Clinical, Cosmetic and Investigational Dermatology. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC10502763/ (Accessed: 22 June 2026).
[7] Ho, C.H., Sood, T. and Zito, P.M. (2025) Androgenetic Alopecia. StatPearls. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC12187474/ (Accessed: 22 June 2026).
[8] Comparison between topical cetirizine with minoxidil versus topical placebo with minoxidil in female androgenetic alopecia: a randomized, double-blind, placebo-controlled study (2023). Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC10205881/ (Accessed: 22 June 2026).
[9] Biotin for Hair Loss: Teasing Out the Evidence (2024), Journal of Clinical and Aesthetic Dermatology. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11324195/ (Accessed: 22 June 2026).
[10] Integral Roles of Specific Proteoglycans in Hair Growth and Hair Loss: Mechanisms behind Proteoglycan Replacement Therapy with Nourkrin with Marilex in Pattern Hair Loss and Telogen Effluvium (2020). Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7222612/ (Accessed: 22 June 2026).
[11] Courier Pharmacy (2026) Comprehensive review of female hair loss: Pathophysiology, treatments, and emerging research. Available at: https://courierpharmacy.co.uk/comprehensive-review-of-female-hair-loss/ (Accessed: 22 June 2026).
[12] Courier Pharmacy (no date) Dutasteride and minoxidil: a powerful combination for hair loss in the UK. Available at: https://courierpharmacy.co.uk/dutasteride-and-minoxidil-a-powerful-combination-for-hair-loss-in-the-uk/ (Accessed: 22 June 2026).
BSc Pharmacy, Independent Prescriber, PgDip Endocrinology, MSc Endocrinology, PgDip Infectious Diseases
Superintendant Pharmacist, Independent Prescriber
BSc Pharmacy
Compounding Pharmacist
